|
Virology vigilance
- an update on MERS and viral mutation and epidemiology
for family doctors
......................................................................................................................................................................
Lesley
Pocock (1)
Mohsen
Rezaeian (2)
(1) Publisher and Medical Educator, medi+WORLD
International, Australia
(2) Professor Mohsen Rezaeian, PhD, Epidemiologist,
Social Medicine Department
Occupational Environmental Research Center, Rafsanjan
Medical School, Rafsanjan University of Medical
Sciences, Rafsanjan, Iran
Correspondence:
Lesley Pocock
medi+WORLD International
Australia
Email:
lesleypocock@mediworld.com.au
|
ABSTRACT
This
paper reviews aspects of virus mutation
and spread generally as well as providing
a review of the major viruses affecting
people in the MENA and MESA regions.
Key words: virus, mutation, Middle East
Respiratory Syndrome (MERS), SARS, Human
Immunodeficiency Virus (HIV), rotavirus,
Chikungunya, Ebola, avian flu, Marburg virus,
rabies, dengue
|
Viruses have been with mankind
and the animal kingdom since recorded history
and their aetiology is still not fully known.
Viruses are not cellular organisms and they may
have either developed separately, or have been
a precursor to cellular life; probably they are
developing 'genetically' according to their own
innate structure.
Throughout history the influenza viruses particularly,
(having connections to simian life), have been
the greatest everyday concern to man and Dengue
viruses also take large numbers of lives in endemic
areas.
Some viruses like smallpox, now eradicated, had
been around for as long as recorded history -
along with childhood viral complaints like rotavirus.
Some scientists believe the Black Death (Bubonic
plague) may have been an Ebola type virus.
While there are viruses specific to humans and
particular animal species, the problematic viruses
have become those that have spread from animals
to humans due to mutation. Some of these mutations
have then gone on to human to human transmission.
Even given better global communications has there
been an actual increase in virus mutation and
spread? In this past 100 years dramatic new viruses
such as HIV, and Ebola, have emerged and spread
rapidly among humans and have caused global concern;
new strains of corona viruses such as SARS and
MERS have been shown to spread rapidly and dramatically
into new populations. We are yet to quantify if
viruses spreading into new host populations may
have an advantage and therefore greater impact
on human health in geographical areas other than
those in which the viruses originated.
The question for scientists and doctors to answer
is, are these outbreaks just part of normal historical
viral epidemiology or do they represent an advanced
state of viral infection due to the virus's own
increased virility or due to, for example, changes
in our biosphere and the ecosphere of carriers
(animals and birds) providing the virus better
access into human hosts. Does human over- population
of the planet, and human's greater proximity to
concentrated animal populations (intensive animal
husbandry) provide a new opportunity for both
development of mutant strains and or the spread
of such mutations globally into human populations
in greater numbers?
If yes, we need to look generally at development
and spread patterns in animal and human hosts
of existing viruses and look equally at the possibility
of development of new strains in certain environments.
It remains an ongoing problem and ongoing work
for doctors, technicians and public health personnel,
as well as global health organisations. Family
doctors who are usually the first contacted and
who live in the patient's local environment where
the outbreak may have originated, particularly
need to be alert not just for evidence and symptoms
of existing strains but for pockets of new viral
strains/mutations.
No part of the world is immune to either locally
developed viral outbreaks or strains of viruses
brought by travellers, or migrant workers into
the local population.
Ideally and with proper scientific application
we should be able to start to pinpoint risk factors/areas
of risk of development of outbreaks (agricultural
areas, specific climatic conditions, migration
paths of wild animal and bird species) and put
in strategies on the community level to contain,
or better, prevent, outbreaks.
In this paper we also provide an update on MERS
and other globally circulating viruses for regional
family doctors who may have patients travelling
to the Hajj, going on Ramadan holidays, and for
those who will see patients who have travelled
from endemic areas overseas.
Accurate estimates of virus mutation
rates are important to understand the evolution
of the viruses and to combat them. However, methods
of estimation are varied and often complex.
The mutation rate is a critical parameter for
understanding viral evolution and has important
practical implications. For example, the estimate
of the mutation rate of HIV-1 demonstrated that
any single mutation conferring drug resistance
should occur within a single day and that simultaneous
treatment with multiple drugs was therefore necessary.
(1)
The viral mutation rate also plays a role in the
assessment of possible vaccination strategies
and it has been shown to influence the stability
of live attenuated polio vaccines. At both the
epidemiological and evolutionary levels, the mutation
rate is one of the factors that can determine
the risk of emergent infectious disease, i.e.,
pathogens crossing the species barrier.
Slight changes of the mutation rate can also determine
whether or not some virus infections are cleared
by the host immune system and can produce dramatic
differences in viral fitness and virulence, clearly
stressing the need to have accurate estimates.
(1)
Future mutation rate studies should fulfil the
following criteria:
- the number of cell infection cycles should be
as low as possible,
- the mutational target should be large,
- mutations should be neutral or lethal or a correction
should be made for selection bias.
Adhering to these criteria will
help us to obtain a clearer picture of virus mutation
patterns. (1)
There have been many laboratory-based
investigations since the emergence of the new
coronaviruses in 2012, but most of the parameters
required for establishing scientifically the control
measures that will protect against them have yet
to be determined. Equally, the global distribution
of the viruses in their animal reservoir has yet
to be established.
The approach to monitoring of
virus mutation is to highlight particular questions
that need to be answered for the purposes of preventing
or treating these infections and diseases.
Table 1: Information required
from investigations for control or mitigation of
a novel respiratory virus affecting humans
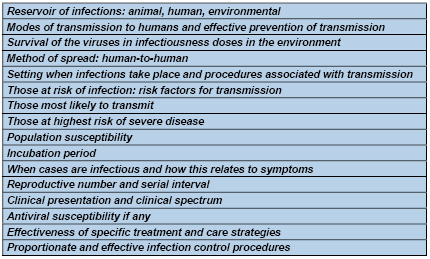
Table 2: What parameters
are involved in virus spread?
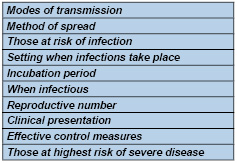
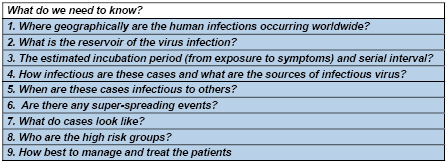
Table 3: Specific public health questions regarding
novel corona viruses that need to be answered
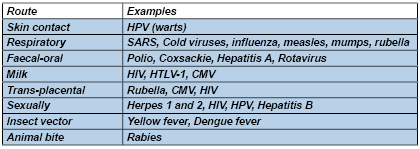
Dealing with virus outbreaks
Viruses cannot exist on their own and for survival
they need to spread to another host. This is because
the original host may either die or eliminate
the infection. Some important routes of viral
transfer include:
|
GLOBAL AND REGIONAL VIRUS UDATES |
MERS
Reproduced with permission
from: World Health Organization
Coronaviruses are a large and
diverse family of viruses that include viruses
that are known to cause illness in humans. MERS-CoV
has never previously been detected in humans or
animals but appears most closely related to coronaviruses
previously found in bats. It is genetically distinct
from the SARS coronavirus, and appears to behave
differently.
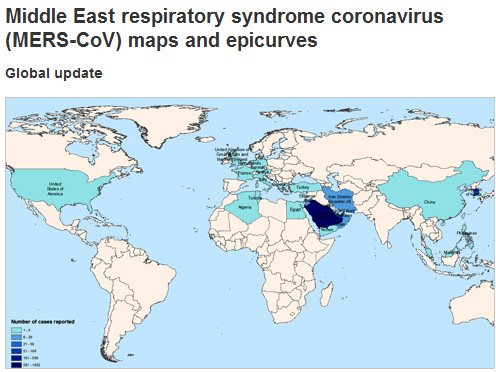
The World Health Organization
(WHO) first reported cases of Middle East Respiratory
syndrome (MERS) coronavirus on 23 September 2012.
While Saudi Arabia has still
recorded the highest number of MERS deaths, (over
400) the outbreak continues in South Korea with
33 deaths and 183 cases to mid June 2015.
All cases have lived in or travelled to the Middle
East, or have had close contact with people who
acquired the infection in the Middle East.
MERS Symptoms
• Most people become unwell quickly, with
fever, cough, shortness of breath, leading to
pneumonia.
• Other symptoms include muscle pain, diarrhoea,
vomiting and nausea.
• There have also been people with mild symptoms
or no symptoms at all. These people had close
contact with others who were seriously ill.
How MERS spreads
• It appears to spread from an infected person
to another person in close contact. The virus
does not appear to spread easily from person-to-person
and appears to spread only from people who are
sick.
• Some people in the Middle East appear to
have caught the disease from infected camels and
bats. How this occurred is not well understood.
People with underlying illnesses that make them
more vulnerable to respiratory disease may be
at a higher risk.
How it is diagnosed
A laboratory test on fluid collected from the
back of the throat or the lungs can diagnose MERS-CoV.
How it is treated
There is no vaccine for MERS-CoV but early and
careful medical care can save lives.
Key facts
• Middle East respiratory syndrome (MERS)
is a viral respiratory disease caused by a novel
coronavirus (MERS-CoV) that was first identified
in Saudi Arabia in 2012.
• Coronaviruses are a large family of viruses
that can cause diseases ranging from the common
cold to Severe Acute Respiratory Syndrome (SARS).
• Typical MERS symptoms include fever, cough
and shortness of breath. Pneumonia is common,
but not always present. Gastrointestinal symptoms,
including diarrhoea, have also been reported.
• Approximately 36% of reported patients
with MERS have died.
• Although the majority of human cases of
MERS have been attributed to human-to-human infections,
camels are likely to be a major reservoir host
for MERS-CoV and an animal source of MERS infection
in humans. However, the exact role of camels in
transmission of the virus and the exact route(s)
of transmission are unknown.
• The virus does not seem to pass easily
from person to person unless there is close contact,
such as occurs when providing unprotected care
to a patient.
Between 1 and 4 June 2015, the National IHR Focal
Point for the Kingdom of Saudi Arabia notified
WHO of 5 additional cases of Middle East respiratory
syndrome coronavirus (MERS-CoV) infection, including
1 death.
Contact tracing of household and healthcare contacts
is ongoing for these cases.
In patients with suspected pneumonia or pneumonitis
with a history of recent residence or travel (in
the 14 days prior to symptom onset) in the Middle
East*, or close contact with confirmed or probable
cases, the following is recommended:
1. The patient should be placed
in a single room if available and standard and
transmission-based precautions implemented (contact,
droplet and airborne), including the use of personal
protective equipment (PPE).
2. The relevant state/territory public health
unit/communicable diseases branch must be notified
urgently of any suspected (and probable or confirmed)
cases in order to discuss patient referral and
coordinate management of contacts.
Note: Transiting through
an international airport (<24hours duration,
remaining within the airport) in the Middle East
is not considered to be risk factor for infection.
Are GPs/FPs at risk from MERS-CoV?
Many confirmed cases have occurred in healthcare-associated
clusters, and there have been a large number of
cases in healthcare workers, but mainly in hospital
settings as has predominantly, if not exclusively,
been the case in South Korea.
The particular conditions or
procedures that lead to transmission in hospital
are not well known. However, lapses in infection
control were known to have occurred for seven
healthcare workers who acquired the infection
from cases in Saudi Arabia.
Patient Pre-travel advice,
travel restrictions, periods of peak travel
The WHO does not currently recommend any restrictions
to travel due to the MERS-CoV outbreak.
Travellers should be aware of the importance of
personal hygiene including frequent hand washing,
avoiding close contact with animals and with people
who are suffering from acute respiratory infection,
and should be advised to seek medical attention
as soon as possible if they feel unwell. They
should also follow usual food hygiene practices
for travellers, including avoiding drinking raw
milk or eating food that may be contaminated with
animal secretions or products unless they are
properly washed, peeled or cooked.
What are the recommended isolation
and PPE recommendations for patients in hospital?
In summary, transmission-based precautions for
suspected, probable and confirmed cases should
include:
• Placement of confirmed and probable cases
in a negative pressure room if available, or in
a single room from which the air does not circulate
to other areas
• Airborne transmission precautions, including
routine use of a P2 respirator, disposable gown,
gloves, and eye protection when entering a patient
care area
• Contact precautions, including close attention
to hand hygiene
• If transfer of the confirmed or probable
case outside the negative pressure room is necessary,
asking the patient to wear a surgical face mask
while they are being transferred and to follow
respiratory hygiene and cough etiquette.
Ebola
Ebola is spread through contact with blood or
other body fluids, or tissue from infected people
or animals. The known strains vary dramatically
in their fatality rates. The Bundibugyo strain
fatality rate is up to 50 percent, and it is up
to 71 percent for the Sudan strain, according
to WHO.
Less than two months after Liberia was declared
Ebola-free by the World Health Organization, the
virus is back in the country.
Even when the outbreak diminished in Liberia,
neighboring Guinea and Sierra Leone have continued
to see 20 to 27 cases a week since late May 2015,
according to the WHO. There have been more than
11,000 total deaths from the outbreak since it
began in March 2014.
Ebola Situation Report
- 8 July 2015
There were 30 confirmed cases of Ebola virus disease
(EVD) reported in the week to 5 July 2015: 18
in Guinea, 3 in Liberia, and 9 in Sierra Leone.
Ebola Situation Report - 1 July 2015
There were 20 confirmed cases of Ebola virus disease
(EVD) reported in the week to 28 June, the same
as the previous week. Weekly case incidence has
been between 20 and 27 cases for 5 consecutive
weeks. In Guinea, 12 cases were reported from
3 prefectures: Boke, Conakry, and Forecariah.
Chikungunya
virus
While not fatal, this virus can
have a chronic disabling effect and it has spread
rapidly around the globe.
Chikungunya is ravaging the Caribbean, having
affected 24 Caribbean nations and possibly more
than 850,000 people worldwide, including 185 Americans
(in New Jerseyans). Chikungunya virus is most
often spread to people by Aedes aegypti and Aedes
albopictus mosquitoes. These are the same mosquitoes
that transmit dengue virus.
• The only way to prevent chikungunya is
to prevent mosquito bites, such as by using repellant.
• Several vaccines are in the developmental
stage but none are in the licensing stage.
• Generally, more South Jersey counties have
a higher risk because they have more Asian Tiger
Mosquitoes.
It is predicted that chikungunya
virus will spread through rest of the globe this
year (2015).
• Prior to 2013, chikungunya virus outbreaks
had been identified in countries in Africa, Asia,
Europe, and the Indian and Pacific Oceans.
• In late 2013, the first transmission of
chikungunya virus in the Americas was identified
in Caribbean countries and territories. Local
transmission means that mosquitoes in the area
have been infected with the virus and are spreading
it to people.
• Since then, local transmission has been
identified in 44 countries or territories throughout
the Americas with more than 1.2 million suspected
cases reported to the Pan American Health Organization
from affected areas.
Symptoms
• Most people infected with chikungunya virus
will develop some symptoms.
• Symptoms usually begin 3-7 days after being
bitten by an infected mosquito.
• The most common symptoms are fever and
joint pain.
• Other symptoms may include headache, muscle
pain, joint swelling, or rash.
• Chikungunya disease does not often result
in death, but the symptoms can be severe and disabling.
• Most patients feel better within a week.
In some people, the joint pain may persist for
months.
• People at risk for more severe disease
include newborns infected around the time of birth,
older adults (>65 years), and people with medical
conditions such as high blood pressure, diabetes,
or heart disease.
• Once a person has been infected, he or
she is likely to be protected from future infections.
SARS
Severe Acute Respiratory Syndrome. No outbreaks
since May 2004 China
Avian
Flu
Avian influenza A (H7N9) is a subtype of influenza
viruses that have been detected in birds in the
past. This particular A (H7N9) virus had not previously
been seen in either animals or people until it
was found in March 2013 in China.
However, since then, infections
in both humans and birds have been observed. The
disease is of concern because most patients have
become severely ill. Most of the cases of human
infection with this avian H7N9 virus have reported
recent exposure to live poultry or potentially
contaminated environments, especially markets
where live birds have been sold. This virus does
not appear to transmit easily from person to person,
and sustained human-to-human transmission has
not been reported.
WHO risk assessment of human
infection with avian influenza A (H7N9) virus
On 23 February 2015 WHO conducted a risk assessment
in accordance with the WHO recommendations for
rapid risk assessment of acute public health events
the summary can be found below.
Risk assessment
This 23 February 2015 risk assessment was conducted
in accordance with WHO's published recommendations
for rapid risk assessment of acute public health
events and will be updated as more information
becomes available.
Overall, the public health risk from avian influenza
A(H7N9) virus has not changed since the assessment
published on 2 October 20142.
What is the likelihood that
additional human cases of infection with avian
influenza A (H7N9) viruses will occur?
The understanding of the epidemiology associated
with this virus, including the main reservoirs
of the virus and the extent of its geographic
spread among animals, remains limited. However,
it is likely that most human cases were exposed
to the H7N9 virus through contact with infected
poultry or contaminated environments, including
markets (official or illegal) that sell live poultry.
Changes to hygiene practices in live poultry markets
have been implemented in many provinces and municipalities.
Since the virus source has not been identified
nor controlled, and the virus continues to be
detected in animals and environments in China,
further human cases are expected in affected and
possibly neighbouring areas.
What is the risk of international spread of
avian influenza A (H7N9) viruses by travellers?
On 27 and 31 Jan 2015, Canada reported 2 cases
of human infection with avian influenza A (H7N9)
in travellers returning from China. These travellers
had mild symptoms and only reported indirect contact
with poultry. On 12 February 2014, Malaysia reported
one human case with avian influenza A (H7N9) virus
infection. The patient was a Chinese resident
who travelled to Malaysia while sick, and was
most likely exposed in China. No further cases
were reported in Malaysia linked to this case.
It is possible that further similar cases will
be detected in other countries among travellers
from affected areas, although community-level
spread in these other countries is unlikely.
Flu viruses
During a typical flu season, up to 500,000 people
worldwide will die from the illness, according
to WHO. But occasionally, when a new flu strain
emerges, a pandemic results with a faster spread
of disease and, often, higher mortality rates.
There are four types of virus
that cause seasonal flu in humans. Every year,
drug developers try to predict which strains are
likely to dominate in the next flu season so as
to create an effective flu vaccine.
A good understanding of the rate and pattern of
virus evolution helps these predictions, as one
of the authors, Dr. Ian Barr, of the World Health
Organization (WHO) Collaborating Centre for Reference
and Research on Influenza in Melbourne, Australia,
explains:
"This work represents another piece in the
complex puzzle of influenza virus circulation
and human infections and provides insights that
will help develop better influenza vaccines that
match strains circulating in the community."
The four viruses that cause seasonal flu in humans
are: influenza A viruses H3N2 and H1N1, and influenza
B viruses Yamagata and Victoria.
The viruses cause similar symptoms - for instance
sudden fever, tiredness and weakness, dry cough,
headache, chills, muscle aches, sore throat -
and they evolve in similar ways.
But what has not been well understood is their
different patterns of spread around the world
and what influences them.
H1N1 and B viruses persist locally between epidemics.
Marburg
virus
Scientists identified Marburg virus in 1967, when
small outbreaks occurred among lab workers in
Germany who were exposed to infected monkeys imported
from Uganda. Marburg virus is similar to Ebola
in that both can cause hemorrhagic fever, meaning
that infected people develop high fevers and bleeding
throughout the body that can lead to shock, organ
failure and death.
The mortality rate in the first outbreak was 25
percent, but it was more than 80 percent in the
1998-2000 outbreak in the Democratic Republic
of Congo, as well as in the 2005 outbreak in Angola,
according to the World Health Organization (WHO).
Rabies
Although rabies vaccines for
pets, which were introduced in the 1920s, have
helped make the disease exceedingly rare in the
developed world, this condition remains a serious
problem in India and parts of Africa.
It destroys the brain, but there is a vaccine
against rabies, and we have antibodies that work
against rabies, so if someone gets bitten by a
rabid animal they can be treated,
If a patient doesn't get treatment, there's a
100 percent possibility they will die.
HIV
In the modern world, the deadliest
virus of all may be HIV. It is still the biggest
killer. An estimated 36 million people have died
from HIV since the disease was first recognized
in the early 1980s.
Powerful antiviral drugs have
made it possible for people to live for years
with HIV. But the disease continues to devastate
many low- and middle-income countries, where 95
percent of new HIV infections occur. Nearly 1
in every 20 adults in Sub-Saharan Africa is HIV-positive,
according to WHO.
Dengue
Dengue virus first appeared in the 1950s in the
Philippines and Thailand, and has since spread
throughout the tropical and subtropical regions
of the globe. Up to 40 percent of the world's
population now lives in areas where dengue is
endemic, and the disease - with the mosquitoes
that carry it - is likely to spread farther as
the world warms.
Dengue sickens 50 to 100 million people a year,
according to WHO. Although the mortality rate
for dengue fever is lower than some other viruses,
at 2.5 percent, the virus can cause an Ebola-like
disease called dengue hemorrhagic fever, and that
condition has a mortality rate of 20 percent if
left untreated.
Rotavirus
Two vaccines are now available to protect children
from rotavirus, the leading cause of severe diarrheal
illness among babies and young children. The virus
can spread rapidly, through what researchers call
the fecal-oral route (meaning that small particles
of feces end up being consumed).
Although children in the developed world rarely
die from rotavirus infection, the disease is a
killer in the developing world, where rehydration
treatments are not widely available.
The WHO estimates that worldwide, 453,000 children
younger than age 5 died from rotavirus infection
in 2008. But countries that have introduced the
vaccine have reported sharp declines in rotavirus
hospitalizations and deaths.
The severity of viral outbreaks
will largely depend on the local, regional and
global response to them. Early vigilance by public
health authorities and family doctors in endemic
areas, particularly, are the greatest preventive
measure along with hygienic practices of people,
especially those living in close proximity to
animal or bird carriers and those in hospital
situations.
Global measures will need to be enacted early
and up to date information made available to limit
spread when it does occur.
Ideally, as in the case of smallpox which was
declared eradicated in 1980 following a global
immunization campaign led by the World Health
Organization, we can start to tackle both the
initial outbreaks and the spread of the more life
threatening viruses.
This takes money and global will.
(1) Nicoll A. Short communication.
Public health investigations required for protecting
the population against novel coronaviruses
(2) WHO Disease Outbreak
(3) http://www.cdc.gov/chikungunya/symptoms/index.html
(4) http://www.who.int/csr/don/en/
(5) Rafael Sanjuán, Miguel R. Nebot, Nicola
Chirico, Louis M. Mansky and Robert Belshaw
Viral Mutation Rates. Journal of Virology. July
2010
|
