|
Low-dose aspirin should be initiated for sickle
cell patients
......................................................................................................................................................................
Mehmet Rami Helvaci (1)
Mustafa Sahan (2)
Feyyaz Bay (1)
Yasin Yildirim (1)
Guner Dede (1)
Emrullah Cihangir (1)
Abdussamet Mermer (1)
Lesley Pocock (3)
(1) Medical Faculty of Mustafa Kemal University,
Department of Internal Medicine, M.D.
(2) Medical Faculty of Mustafa Kemal University,
Department of Emergency Medicine, M.D.
(3) medi+WORLD International
Correspondence:
Mehmet Rami Helvaci, M.D.
Medical Faculty of the Mustafa Kemal University,
31100, Serinyol, Antakya, Hatay, TURKEY
Phone: 00-90-326-2291000 (Internal 3399) Fax:
00-90-326-2455654
Email: mramihelvaci@hotmail.com
|
ABSTRACT
Background: We tried to understand
whether or not there is an association between
platelet (PLT) count of peripheric blood
and severity of sickle cell diseases (SCDs).
Methods: SCDs patients with red blood
cell (RBC) transfusions of less than 50
units in their lives were put into the first
and 50 units or higher were put into the
second groups.
Results: The study included 224 patients
(70.8%) in the first and 92 patients (29.1%)
in the second groups (p<0.001). Mean
ages were similar in both groups (28.9 and
30.0 years, respectively, p>0.05). Male
ratio was significantly higher in the second
group (45.5% versus 64.1%, p<0.001).
Although smoking was also higher in the
second group (12.0% versus 17.3%, p>0.05),
the difference was nonsignificant probably
due to the small sample size of the second
group. Mean units of transfused RBCs were
12.9 and 99.0 in the groups (p<0.000).
Although white blood cell and PLT counts
of peripheric blood were higher in the second
group, the difference was only significant
for the PLT counts (p= 0.005), probably
due to the same reason above. Number of
painful crises per year, digital clubbing,
chronic obstructive pulmonary disease, leg
ulcers, stroke, chronic renal disease, and
coronary heart disease were higher in the
second group, significantly (p<0.05 for
all).
Conclusion: SCDs are chronic inflammatory
processes on endothelium mainly at the capillary
level, and there was a highly significant
association between PLT count and severity
of the SCDs. So low-dose aspirin will probably
be beneficial for patients with SCDs.
Key words: Sickle cell diseases,
low-dose aspirin, chronic endothelial damage,
atherosclerosis
|
Atherosclerosis may be the major
cause of aging by inducing tissue hypoxia all
over the body. For example, cardiac cirrhosis
develops due to the prolonged hepatic hypoxia
in patients with pulmonary and/or cardiac diseases.
Probably whole afferent vasculature including
capillaries are involved in the process. Some
of the currently known accelerator factors of
the obliterative process are physical inactivity,
overweight, and smoking for the development of
irreversible consequences including obesity, hypertension,
diabetes mellitus (DM), peripheric artery disease
(PAD), chronic obstructive pulmonary disease (COPD),
chronic renal disease (CRD), coronary heart disease
(CHD), cirrhosis, mesenteric ischemia, osteoporosis,
and stroke, all of which terminate with early
aging and death. They were researched under the
title of metabolic syndrome in the literature,
extensively (1-3). Similarly, sickle cell diseases
(SCDs) are chronic inflammatory processes on endothelium
mainly at the capillary level. Hemoglobin S (HbS)
causes loss of elastic and biconcave disc shaped
structures of red blood cells (RBCs). Probably,
loss of elasticity instead of shapes of RBCs is
the major problem, since sickling is very rare
in the peripheric blood samples of the SCDs patients
with associated thalassemia minors, and human
survival is not so affected in hereditary elliptocytosis
or spherocytosis. Loss of elasticity is probably
present in whole lifespan, but it is exaggerated
with increased metabolic rate of the body. The
hardened cells induced prolonged endothelial inflammation,
edema, remodeling, and fibrosis mainly at the
capillary level terminate with disseminated tissue
infarcts all over the body (4,5). On the other
hand, obvious vascular occlusions may not develop
in greater vasculature due to the transport instead
of distribution function of them. We tried to
understand whether or not there is an association
between platelet (PLT) count of peripheric blood
and severity of SCDs in the present study.
The study was performed in Medical
Faculty of the Mustafa Kemal University between
March 2007 and January 2014. All patients with
the SCDs were enrolled into the study. SCDs are
diagnosed by the hemoglobin electrophoresis performed
via high performance liquid chromatography (HPLC).
Their medical histories including numbers of painful
crises per year, mean units of transfused RBC
in their lives, smoking habit, regular alcohol
consumption, leg ulcers, and stroke were learnt.
Cases with a history of one pack-year were accepted
as smokers, and one drink-year were accepted as
drinkers. A check up procedure including serum
iron, iron binding capacity, ferritin, creatinine,
liver function tests, markers of hepatitis viruses
A, B, and C and human immunodeficiency virus,
a posterior-anterior chest x-ray film, an electrocardiogram,
a Doppler echocardiogram, an abdominal ultrasonography,
a computed tomography of brain, and a magnetic
resonance imaging (MRI) of hips was performed.
Other bones for avascular necrosis were scanned
according to the patients' complaints. So avascular
necrosis of bones was diagnosed by means of MRI
(6). Cases with acute painful crises or any other
inflammatory event were treated at first, and
then the laboratory tests and clinical measurements
were performed on the silent phase. Stroke is
diagnosed by the computed tomography of brain.
The criterion for diagnosis of COPD is post-bronchodilator
forced expiratory volume in 1 second/forced vital
capacity of less than 70% (7). CRD is diagnosed
with a permanent creatinine level of 1.3 mg/dL
or higher in males and 1.2 mg/dL or higher in
females during the silent period. Cirrhosis is
diagnosed with liver function tests, ultrasonographic
findings, and histologic procedure in case of
indication. Digital clubbing is diagnosed with
the ratio of distal phalangeal diameter to interphalangeal
diameter which is greater than 1.0 and with the
presence of Schamroth's sign (8,9). Associated
thalassemia minors are detected with serum iron,
iron binding capacity, ferritin, and hemoglobin
electrophoresis performed via HPLC. A stress electrocardiography
is performed just for cases with an abnormal electrocardiogram
and/or angina pectoris. Coronary angiography is
taken just for the stress electrocardiography
positive cases. So CHD was diagnosed either angiographically
or with the Doppler echocardiographic findings
as the movement disorders in the cardiac walls.
Eventually, cases with RBC transfusions of less
than 50 units in their lives were put into the
first and 50 units or higher were put into the
second groups, and the groups were compared in
between. Mann-Whitney U test, Independent-Samples
t test, and comparison of proportions were used
as the methods of statistical analyses.
Table 1: Sickle cell patients
with the units of red blood cell transfusions
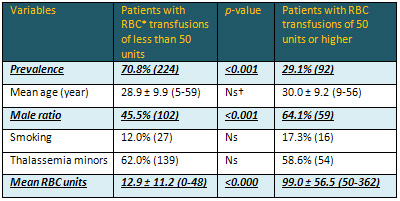
*Red blood cell †Nonsignificant (p>0.05)
Table 2: Sickle cell patients with peripheric
blood values
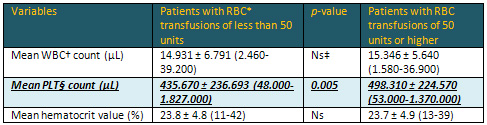
*Red blood cell †White blood cell ‡Nonsignificant
(p>0.05) §Platelet
Table 3: Sickle cell patients with associated
disorders

*Red blood cell †Nonsignificant (p>0.05)
‡Chronic obstructive pulmonary disease §Chronic
renal disease Coronary heart disease
The study included 316 patients with the SCDs
(155 females and 161 males). There were 224 patients
(70.8%) in the first and 92 patients (29.1%) in
the second groups (p<0.001). The mean ages
of the groups were similar (28.9 and 30.0 years,
respectively, p>0.05). Interestingly, the male
ratio was significantly higher in the second group
(45.5% versus 64.1%, p<0.001). Although the
prevalence of smoking was also higher in the second
group (12.0% versus 17.3%), the difference was
nonsignificant probably due to the small sample
size of the second group (p>0.05). There was
a nonsignificant difference according to the prevalence
of associated thalassemia minors (p>0.05).
The mean units of transfused RBCs were 12.9 and
99.0 in the first and second groups, respectively
(p<0.000) (Table 1). Although both the WBC
and PLT counts of the peripheric blood were higher
in the second group, the difference was only significant
for the PLT counts (p= 0.005), probably due to
the small sample size of the second group again.
Mean hematocrit values were similar in the first
and second groups (23.8% versus 23.7%, respectively,
p>0.05) (Table 2). Although the prevalences
of avascular necrosis of bones, cirrhosis, and
exitus were similar in both groups (p>0.05
for all), the mean number of painful crises per
year, digital clubbing, COPD, leg ulcers, stroke,
CRD, and CHD were significantly higher in the
second group (p<0.05 for all) (Table 3). Mean
ages of the mortal cases were 29.5 ± 9.8
(19-50) and 34.6 ± 6.7 (26-44) years in
the first and second groups, respectively (p>0.05).
Mean ages of the mortal cases were 29.7 ±
9.6 (19-50) and 33.3 ± 8.5 (21-44) years
in males and females, respectively (p>0.05).
On the other hand, there was no patient with regular
alcohol consumption among the study cases. Although
antiHCV was positive in two of the cirrhotics,
HCV RNA was detected as negative by polymerase
chain reaction in both.
Chronic endothelial damage and
atherosclerosis is the most common type of vasculitis,
and the leading cause of morbidity and mortality
in elderlies. Probably whole afferent vasculature
including capillaries are involved in the body.
Much higher BP of the afferent vasculature may
be the major underlying cause, and efferent vessels
are probably protected due to the much lower BP
in them. Secondary to the prolonged endothelial
damage and fibrosis, vascular walls become thickened,
their lumens are narrowed, and they lose their
elastic natures which can reduce the blood flow
and increase BP further. Although early withdrawal
of the causative factors including smoking, physical
inactivity, excess weight, increased serum glucose
and lipids, and elevated arterial BP may prevent
terminal consequences, after development of COPD,
cirrhosis, CRD, CHD, PAD, or stroke, the endothelial
changes may not be reversed completely due to
the fibrotic natures of them (10).
SCDs are life-threatening genetic
disorders affecting nearly 100.000 individuals
in the United States (11). As a difference from
other causes of atherosclerosis, the SCDs probably
keep vascular endothelium mainly at the capillary
level (12), since the capillary system is the
main distributor of the hardened RBCs to tissues.
The hardened cells induced chronic endothelial
damage, inflammation, edema, and fibrosis build
up an advanced atherosclerosis in much younger
ages. As a result, the lifespans of patients with
the SCDs were 48 years in females and 42 years
in males in the literature (13), whereas they
were 33.3 and 29.7 years in the present study,
respectively. The great differences may be secondary
to delayed initiation of hydroxyurea therapy and
inadequate RBC transfusions in emergencies in
our country. On the other hand, longer lifespan
of females with the SCDs and longer overall survival
of females in the world can not be explained by
the atherosclerotic effects of smoking alone,
instead it may be explained by physical power
requiring role of male sex in life (14,15), since
physical power induced increased metabolic rate
may terminate with an exaggerated sickling and
atherosclerosis in human body.
Painful crises are nearly pathognomonic for the
SCDs, and precipitated by infections, operations,
depressions, and disseminated tissue damage. Although
painful crises may not be life threatening directly
(16), increased metabolic rate may terminate with
multiorgan failures on the chronic inflammatory
background of the SCDs (17). The severe pain may
be secondary to the disseminated inflammation
of the capillary endothelium, and the increased
WBC and PLT counts and decreased hematocrit values
may show presence of a chronic inflammatory process
during whole their lives in such patients in the
present study. Similar to us, increased WBC counts
even in the absence of a painful crisis was an
independent predictor of the disease severity
(18), and it was associated with an increased
risk of stroke by causing disseminated endothelial
damage in brain (19). Due to the severity of pain,
narcotic analgesics are usually required (20),
but according to our experiences, simple and repeated
RBC transfusions are highly effective during the
severe crises both to relieve pain and to prevent
sudden death that may develop secondary to the
multiorgan failures on the chronic inflammatory
background of the SCDs. Simplicity of preparation
of RBC suspensions in a short period of time provides
advantages to clinicians to use them even in small
public hospitals without the requirement of specialized
health workers and equipments as in RBC exchange.
Additionally, preparation of one or two units
of RBC suspension in each time provides time to
clinicians to prepare more units by preventing
sudden death of the patients. By this way, we
can prevent some of deaths developed during transport
of severe cases to tertiary health centers.
Hydroxyurea is an effective drug in chronic myeloproliferative
disorders and SCDs (12). It interferes with cell
division by blocking the formation of deoxyribonucleotides
which are building blocks of DNA. Although the
action way of hydroxyurea is thought to be the
increase of gamma globin synthesis for fetal hemoglobin
(HbF) (21,22), its main action may be suppression
of hyperproliferative WBC and PLTs in the SCDs.
As in autoimmune disorders, although presence
of a continuous damage of hardened RBCs on endothelium,
the severity of endothelial destruction is probably
exaggerated by the patients' own WBCs and PLTs
in the SCDs. Due to the same action way, hydroxyurea
is also used in moderate and severe psoriasis
to suppress hyperproliferative skin cells. Similarly,
lower neutrophil counts were associated with lower
crisis rates, and if a tissue infarction occurs,
lower neutrophil counts may limit severity of
pain and extent of tissue damage (23). On the
other hand, final HbF levels in hydroxyurea users
did not differ from their pretreatment levels,
significantly (23). Similarly, the Multicenter
Study of Hydroxyurea studied 299 severely involved
adults with sickle cell anemia (HbSS), and compared
the results of patients treated with hydroxyurea
or placebo (24). The study especially searched
effects of the drug on painful crises, acute chest
syndrome, and requirement of RBC transfusions.
The results were so overwhelming in the favour
of hydroxyurea that the study was terminated after
22 months, and hydroxyurea was initiated to all
patients. The patients treated with hydroxyurea
had a 44% decrease of hospitalizations, and there
was an independent association of lower neutrophil
counts with the lower crisis rates (24). But this
study was performed in severe HbSS cases alone,
and the mean number of painful crises was decreased
from 4.5 to 2.5 per year (24). Whereas in one
of our studies, we studied 337 patients with all
subtypes and severities of the SCDs, and the mean
number of painful crises was decreased from 10.3
to 1.7 per year (p<0.000) with an additional
decreased severity of them (7.8 versus 2.2, degree
of severity according to patient's self-explanation
between 0 and 10, p<0.000) (25). Additionally,
adult SCDs patients using hydroxyurea appear to
have a reduced mortality rate after a 9-year follow-up
period (26). Although the underlying disease severity
remains critical to determine prognosis, hydroxyurea
may decrease severity of disease (26) and prolong
survival (12). Furthermore, infants with lower
hemoglobin levels were more likely to have higher
incidences of acute chest syndrome, painful crises,
and lower neuropsychological scores, and hydroxyurea
reduced the incidences of them (27). Hydroxyurea
in early years of life may also protect splenic
function, improve growth, and prevent multiorgan
dysfunctions. Transfusion programmes can also
reduce the complications, but they carry some
major risks including infections, development
of allo-antibodies, and iron overload. Beside
that, using an oral drug is a much more easier
method than the regular blood transfusions for
the patients, families, health workers, and insurance
systems.
Aspirin is a nonsteroidal anti-inflammatory drug
(NSAID), but differs from most others in the mechanism
of action, since only low-doses of aspirin (75-100
mg/day) exert protective vascular effects (28).
Although aspirin and other salicylates have similar
effects (analgesic, antipyretic, and anti-inflammatory)
with the other NSAIDs and inhibit the same enzyme
cyclooxygenase (COX), aspirin does so in an irreversible
manner and, unlike others, affects more the COX-1
than the COX-2 variants of the enzyme. It inhibits
the production of thromboxane, which is significant
for building of a patch over damaged blood vessels.
Because the patch can become too large and block
blood flow extensively, aspirin is also used at
low-doses to prevent heart attacks, strokes, and
other thromboembolic events. Additionally, low-doses
of aspirin are usually given just after a heart
attack to reduce the risk of progression or development
of others. A review of data regarding aspirin
use for secondary prevention of acute coronary
syndromes demonstrated that low-doses of aspirin
are consistently favored for short- and long-term
use due to the lack of a dose-response relationship
between increasing the dose and improved efficacy,
and a higher incidence of gastrointestinal bleeding
with increasing the dose (28,29). Women aged 65
years and older without any established cardiovascular
disease, women of any age with established cardiovascular
disease, and women of any age with an estimated
10-year risk of cardiovascular disease of 10%
or higher are likely to experience a benefit from
low-doses of aspirin (30). Low-doses of aspirin
have been shown to be effective in prevention
of one-fifth of thromboembolic events (non-fatal
myocardial infarction, non-fatal stroke, or vascular
death) in a meta-analysis of 16 secondary prevention
trials in patients with previous myocardial infarction,
stroke, or transient cerebral ischemia. This corresponds
to an absolute reduction of about 10-20 per 1.000
patients in the yearly incidence of non-fatal
events, and to a smaller, but still definite,
reduction in vascular death (31). So the benefits
of antiplatelet therapy substantially exceed the
risk for secondary prevention (31), and use of
low-doses of aspirin reflects good clinical practice
and is encouraged in current guidelines (29).
As a conclusion, SCDs are chronic inflammatory
processes on endothelium mainly at the capillary
level and there was a highly significant association
between PLT count and severity of the SCDs. So
low-dose aspirin will probably be beneficial for
patients with the SCDs.
1. Eckel RH, Grundy SM, Zimmet
PZ. The metabolic syndrome. Lancet 2005; 365:
1415-1428.
2. Helvaci MR, Kaya H, Duru M, Yalcin A. What
is the relationship between white coat hypertension
and dyslipidemia? Int Heart J 2008; 49: 87-93.
3. Helvaci MR, Kaya H, Seyhanli M, Yalcin A. White
coat hypertension in definition of metabolic syndrome.
Int Heart J 2008; 49: 449-457.
4. Helvaci MR, Aydogan A, Akkucuk S, Oruc C, Ugur
M. Sickle cell diseases and ileus. Int J Clin
Exp Med 2014; 7: 2871-2876.
5. Helvaci MR, Acipayam C, Aydogan A, Akkucuk
S, Oruc C, Gokce C. Acute chest syndrome in severity
of sickle cell diseases. Int J Clin Exp Med 2014;
7: 5790-5795.
6. Mankad VN, Williams JP, Harpen MD, Manci E,
Longenecker G, Moore RB, et al. Magnetic resonance
imaging of bone marrow in sickle cell disease:
clinical, hematologic, and pathologic correlations.
Blood 1990; 75: 274-283.
7. Global strategy for the diagnosis, management
and prevention of chronic obstructive pulmonary
disease 2010. Global initiative for chronic obstructive
lung disease (GOLD).
8. Schamroth L. Personal experience. S Afr Med
J 1976; 50: 297-300.
9. Vandemergel X, Renneboog B. Prevalence, aetiologies
and significance of clubbing in a department of
general internal medicine. Eur J Intern Med 2008;
19: 325-329.
10. Helvaci MR, Aydin LY, Aydin Y. Digital clubbing
may be an indicator of systemic atherosclerosis
even at microvascular level. HealthMED 2012; 6:
3977-3981.
11. Yawn BP, Buchanan GR, Afenyi-Annan AN, Ballas
SK, Hassell KL, James AH, et al. Management of
sickle cell disease: summary of the 2014 evidence-based
report by expert panel members. JAMA 2014; 312:
1033-1048.
12. Helvaci MR, Aydin Y, Ayyildiz O. Hydroxyurea
may prolong survival of sickle cell patients by
decreasing frequency of painful crises. HealthMED
2013; 7: 2327-2332.
13. Platt OS, Brambilla DJ, Rosse WF, Milner PF,
Castro O, Steinberg MH, et al. Mortality in sickle
cell disease. Life expectancy and risk factors
for early death. N Engl J Med 1994; 330: 1639-1644.
14. Mathers CD, Sadana R, Salomon JA, Murray CJ,
Lopez AD. Healthy life expectancy in 191 countries,
1999. Lancet 2001; 357: 1685-1691.
15. Helvaci MR, Ayyildiz O, Gundogdu M. Gender
differences in severity of sickle cell diseases
in non-smokers. Pak J Med Sci 2013; 29: 1050-1054.
16. Parfrey NA, Moore W, Hutchins GM. Is pain
crisis a cause of death in sickle cell disease?
Am J Clin Pathol 1985; 84: 209-212.
17. Helvaci MR, Gokce C. Painful crises and survival
of sickle cell patients. HealthMED 2014; 8: 598-602.
18. Miller ST, Sleeper LA, Pegelow CH, Enos LE,
Wang WC, Weiner SJ, et al. Prediction of adverse
outcomes in children with sickle cell disease.
N Engl J Med 2000; 342: 83-89.
19. Balkaran B, Char G, Morris JS, Thomas PW,
Serjeant BE, Serjeant GR. Stroke in a cohort of
patients with homozygous sickle cell disease.
J Pediatr 1992; 120: 360-366.
20. Cole TB, Sprinkle RH, Smith SJ, Buchanan GR.
Intravenous narcotic therapy for children with
severe sickle cell pain crisis. Am J Dis Child
1986; 140: 1255-1259.
21. Miller BA, Platt O, Hope S, Dover G, Nathan
DG. Influence of hydroxyurea on fetal hemoglobin
production in vitro. Blood 1987; 70: 1824-1829.
22. Platt OS. Is there treatment for sickle cell
anemia? N Engl J Med 1988; 319: 1479-1480.
23. Charache S. Mechanism of action of hydroxyurea
in the management of sickle cell anemia in adults.
Semin Hematol 1997; 34: 15-21.
24. Charache S, Barton FB, Moore RD, Terrin ML,
Steinberg MH, Dover GJ, et al. Hydroxyurea and
sickle cell anemia. Clinical utility of a myelosuppressive
"switching" agent. The Multicenter Study
of Hydroxyurea in Sickle Cell Anemia. Medicine
(Baltimore) 1996; 75: 300-326.
25. Helvaci MR, Ayyildiz O, Gundogdu M. Hydroxyurea
therapy and parameters of health in sickle cell
patients. HealthMED 2014; 8: 451-456.
26. Steinberg MH, Barton F, Castro O, Pegelow
CH, Ballas SK, Kutlar A, et al. Effect of hydroxyurea
on mortality and morbidity in adult sickle cell
anemia: risks and benefits up to 9 years of treatment.
JAMA 2003; 289: 1645-1651.
27. Lebensburger JD, Miller ST, Howard TH, Casella
JF, Brown RC, Lu M, et al; BABY HUG Investigators.
Influence of severity of anemia on clinical findings
in infants with sickle cell anemia: analyses from
the BABY HUG study. Pediatr Blood Cancer 2012;
59: 675-678.
28. Soubrier M, Rosenbaum D, Tatar Z, Lahaye C,
Dubost JJ, Mathieu S. Vascular effects of nonsteroidal
antiinflammatory drugs. Joint Bone Spine 2013;
80: 358-362.
29. Berger JS. Aspirin, clopidogrel, and ticagrelor
in acute coronary syndromes. Am J Cardiol 2013;
112: 737-745.
30. Manson JE, Bassuk SS. When is the use of aspirin
for CVD prevention in women appropriate? Menopause
2014; 21: 103-105.
31. Patrono C. Low-dose aspirin in primary prevention:
cardioprotection, chemoprevention, both, or neither?
Eur Heart J 2013; 34: 3403-3411.
|
