|
Art of killing?
......................................................................................................................................................................
Safaa
Bahjat
Correspondence:
Dr Safaa Bahjat
Kirkuk, Iraq
Email:
dr.safaabahjat@hotmail.com
......................................................................................................................................
Iraq within
the past three decades has been subjected to 3
large wars and to off and on military episodes
in between. Recently another open end war was
launched against the ISIS and the output is the
same: senseless killing, abject suffering, large-scale
displacement , and unprecedented destruction are
occurring every day .The daily bloodshed devalues
all people, not just those directly engulfed in
it. This realization contradicts the guilt-relieving
notion that there is nothing to be done.
With bitterness we recall the 23rd anniversary
of the Desert storm battle outbreak and particularly
the crime of using Depleted Uranium (DU)which
was potentially involved in the recent upsurge
of malignancies in populations exposed to war
dust.
It is well-known that weapons
containing natural uranium (NU), that is, 'nuclear
weapons' are
disqualified due to their radioactivity, prompt
mass destructive power, and long lasting genotoxicity,
which has a sustained effect through generations.
However, as DU has not been globally and legally
well-identified and studied, and as it formed
a heavy disposal task on the nuclear industry,
this allowed it to leak to the traditional weapon
industry for deeper destructive effects instead
of being buried costly in nuclear graveyards.
In light of new reports tackling the disastrous
outcome of DU on the health of exposed populations,
a question arises, as to which extent may the
weapons containing DU yet be considered conventional,
and does DU still retain similarities with the
"maternal" NU, regarding the toxic and
carcinogenic effect, which the latter has. It
is important here to be reminded of the biodata
of NU and DU. On average, approximately 90 (micrograms)
of uranium exists normally in the human body,
this is gained from normal intakes of water, food,
and air. Approximately 66% is found in the skeleton,
16% in the liver, 8% in the kidneys, and 10% in
other tissues. (http://www.who.int/mediacentre/factsheets/fs257/en)
However, DU is a nuclear exhaust born as a byproduct
of Uranium impregnation in the nuclear industry,
and almost completely formed from Uranium-238
(U238),which has a 60% radiation power of NU.
Physically, NU and DU consist of a mixture of
3 radioactive isotopes but in different ratios;
NU contains U238 (99.27% by mass), U235 (0.72%),
and U234 (0.0054%), whereas DU contains approximately
99.8% U238, 0.2% U235, and 0.001% U234 by mass.
The main difference between DU and NU is that
the former contains at least 3 times less U235
than the latter. Table 1 shows the half-lives
and the specific activity of the 3 isotopes of
NU and DU, the average energies per transformation
emitted by these isotopes, and the percentages
of isotopic abundance by weight and activity of
NU and DU. (Data derived from URL: http://www.who.int/mediacentre/factsheets/fs257/en).
The DU behaves chemically, physically,
and toxicologically similar to NU. As it was found
to still retain an extra penetrative and destructive
effect, it is presently involved in the manufacture
of high-powered
smart bullets/missiles, and thus it entered the
armory of the arsenal as an anti-tank shell agent.
Uranium-238 is pyrophoric, bursting after shooting
into flame with 70% of the shell aerosolized into
respirable particles less than 5 microns in diameter.
Most DU particles are dispersed as dust on earth,
which when it rains, penetrates into the soil
to contaminate water resources, and consequently
agricultural products. Uranium-238 is an alpha
radioactive emitter. On degradation, it shoots
mainly alpha, and to a lesser quantity beta particles.
Man, in and around the battle field, is exposed
to DU hazards by radiation, inhalation, swallowing,
and wound contamination. In the human body, DU
is nephro-toxic; it is mostly excreted via the
kidney causing acute nephritis, however, it is
also excreted in the semen, and uranyl ions infiltrate
the testes, ovaries, placenta, embryo, and central
nervous system. Naturally, children are more susceptible
to radiation induced cancers than adults.
A mainstay report published in Saudi Medical Journal
in 2003 by Al-Waiz et al from Baghdad University
clearly shows that (Kaposi Sarcoma) KS has recently
made an upsurge in southern Iraq, and it behaved
in these particular cases quite divergently compared
with the well-known classic KS, which existed
before sporadically in Middle Eastern people including
Iraqis. The report concluded that this KS outbreak
might have been provoked and/or boosted by DU
fallout. The differences between the new Iraqi
KS outbreak and the known classic type may be
concluded in:
1. Age: the mean age of patients in these
series was 54 years compared with 68 years in
classic KS, thus these patients were 14 years
younger than the classic KS patients, that is,
14 years earlier presentation.
2. Advanced presentation: classic KS usually
presents as macular lesions and progresses very
slowly to plaques or nodules, but the disease
in all these patients presented directly in the
advanced plaque and nodular stage, none was in
the macular stage. This is a major deviation from
the classic KS, which suggests a rather aggressive
nature, and more rapid course probably related
to a new potential factor.
3. Visceral involvement: KS patients (25%)
had lung and liver involvement, and 10% of them
had lymph node involvement within a short period
of the disease course. Considering that the visceral
dissemination occurs very lately and infrequently
in classic KS reflects again a comparatively more
florid type of KS than the classic one.
4. High mortality rate: The mortality rate
was 15%, and death was due to systemic dissemination
of the tumor. Whereas, classic KS patients enjoy
a rather normal life span, approximately 10-20
years in average and death is very rarely related
to KS.5. The southern geographic predilection:
one case of KS only came from northern Iraq, which
is comparatively calm and far from the battle
field, versus 15 cases that came from the central
Baghdad region, and 4 that came from the south;
this suggests some geographical polarization of
KS distribution consistent with the battle field
- Baghdad and south Iraq. Considering that Baghdad
is relatively closer to the south increases the
polarization to one case north versus 19 middle/south.
This southern:northern ratio of KS cases is far
bigger than that of the populace distribution.
The northern people alone are approximately 8
million. From the Wikipedia almost 75% of Iraq's
population lives in the flat, alluvial plain stretching
southeast from Baghdad to Basra, and the Arabian
Gulf. Possibly, approximately one quarter of Iraqi
population lives in the north, and one KS case
came only from the North, and 19 from the Midsouth.
This inconsistent geographical distribution of
KS cases which are not parallel with the populace
distribution suggests a Southern related factor
incriminated in KS epidemic, and it existed in
the Middle South, that is the focus of the battle
field during successive wars. 6. The epidemic
occurrence: This is highlighted via a cluster
of 20 KS cases diagnosed within a short (one year)
period, and perhaps, this number has jumped up
later. Literature review shows that this compact
episode of KS is probably the first recorded in
Iraq, and in all the neighboring countries. Fortunately,
there was an Iraqi study of 21 cases of classic
KS 15 years before, that is, before the Gulf war
era but with a quite different clinical behavior.
Thus, the current report involves almost the same
number of patients but within a tenth of the period
of the previous study.
Reports from southern Iraq have documented a steep
rise in the incidence of cancers since the 1990s,
especially in children. According to the Cancer
Treatment Centre of Basra, in the far Southern
Iraq and the focus of the Gulf wars, local cancer
incidence raised from 11 cancers per 100,000 in
1988 to 75 in 1998, and 116 in 2001, approximately
11 fold in 13 years, rising almost one fold each
year. In Fallujah, Busby et al found that the
results qualitatively support the existence of
serious mutation-related health effects as 80
deaths per 1,000 births were reported in Fallujah
compared with only19.8 in Egypt. Caldicott recalled
the mechanisms, by which depleted uranium induces
mutations and cell damage. Cells are attacked
directly and indirectly by DU. The alpha rays
hit the DNA molecules resulting in direct damage
to the chromosomes, although this damage is not
stationary, it passes via generations posing genomic
instability of the damaged cells. Additionally
indirect bystander effect occurs to the intact
adjacent cells by uranyl ions, which bind avidly
to DNA-clumped chromatin causing DNA damage and
chemical toxicity, hence, their mutagenic capability.
Hamilton inquires why adequate measures were not
taken to ensure that good scientific evidence
for later use was obtained at the onset of both
Gulf and Balkan conflicts. It is possible that
at the time of confrontations, circumstances were
not fit, there were political or military limits,
which made the recurrent publication and media
comments on these events decades after their occurrence
just serve in dissolving the confidence of the
general public. Possible, however the lack of
publication and media coverage serves also to
obscure the problem rather than solving them,
whereas it continues to exist inconspicuously
with extra potential human sufferers. For fairness,
it is worth mentioning that some studies showed
leniency with DU and did not refuse using it in
military, for instance, Patel in his article "Health
in the Middle East: No strong link between depleted
uranium and cancer", and McDiarmid ("Depleted
uranium and public health. Fifty years study of
occupational exposure provides little evidence
of cancer") but circumstances of both are
quite different. Uncontrolled occupational exposure
is quite different from haphazard permanent residence
of the whole society, including children and pregnant
women inside the contaminated field. Yet, the
authors could not deny the existence of an insidious
link or evidence of malignant relation between
DU and cancer, the term they used -no strong "link"
- and -little "evidence" - ascertains
the presence of a "link" with, and an
evidence of cancer rather than denying it.
It is not the size of the "evidence"
or the "link" between DU and cancer
which accounts in human affairs, but the link
itself; it is incriminated even if it kills one
man only. Size can act in the field of materials
not in humans.
We, in the medical field
feel it is part of our medical mission and educational
deputation as pioneering medical media in the
region, to notify any malpractice against human
health or life, share in protecting the common
people from mass health disruption, and send a
plea to whom it may concern, such as the WHO,
United Nations, the Green Groups, and all concerned
health authorities requesting them to consider
research reports regarding KS originated from
the Gulf and Balkan region as work paper, which
is worthy of further investigation and follow
up, that is:
1. Perform epidemiological studies with
control groups and further mass population screening
for any uprise in mortality and morbidity in general,
and malignancy in particular and around the battle
fields, prospectively and retrospectively, to
document the old cases and discover the new ones
as early as possible in order to have a larger
statistical database to depend on in the next
steps.
2. Perform further in vitro laboratory
research and animal studies -although not ideal
with battle field medium to
clear any suspicion regarding DU - human health
relation on radiological, toxic, and molecular
basis. 3. Until a final conclusion is issued,
to ban the use of DU in any means until full knowledge
of its safety and
hazards is evident. Military experts should obtain
a safety certificate of DU before taking it to
the field but not after. Safety should never be
proved retrospectively or provisionally, as long
as man is not a laboratory rat to start with in
death trials, and as long as prevention is better
than cure as we always say, noticing that once
DU is blasted, it will never vanish, it will finally
pollute the water, agriculture, and human life
in an everlasting circle.
International health authorities who care should
undergo regular check up on the factories of death
materials to see what is up, they should not wait
and see, but should move -prophylactic wise- there
to face the death engineers in the pre-manufacturing
stage in order to control the obsessive killing
drive in that media, and suppress the explosive
fatal craving. Performing all these preventive
measures is crucial -particularly at this very
time with new launch of wars, in order to clear
the relation between DU and uprising malignancies,
and to clean this perpetual hazardous contaminant
of human life. When NU is disqualified for its
non-conventional mass destructive effect, DU with
60% radiation of NU, and with everlasting environmental
contaminating effect is a genuine suspect, it
should not at all be justified and passed, and
should not be simply considered as conventional
until proven otherwise by unbiased evidence-based
science. There seems to be a thick wall separating
militarists and health preachers. Each is working
separately and independently, one with death and
the other against it, without minimal coordination
and harmony. This wall should be knocked down
so that they might work together like a smart
surgical team when this does a legal operation.
Yes, bombs are made to kill, but they should not
do this randomly, they should first earn a health
certificate before going to war and before killing.
Materials involved in them should not be used
until safety measures are confirmed, and preserved
in terms of effects, adverse effects, and contra
effects, exactly like poisons, and pharmaceutical
materials. The side effects of these materials
are as vital as the effects .In fact, they are
effects on the long run. In another way, they
should not kill massively beyond the range of
their pre-decided legal claw, and "hiddenly"
through mutagenicity, which works deeply across
decades and generations. In terms of DU, allow
the manufacturers to first prove its conventionality
and then use it, but not before. The capacity
of death should be callipered precisely in extent,
mass and duration so that no undesirable hidden
killing would silently take place. Illegal instruments
should not be used, even in killing, although
the taste of death is finally alike. Instruments
also should be compatible with -but not above-
the morals and ethics of wars, and nothing should
be there above ethics and norms.
Leaving a sustained agendum of death to act insidiously
and deeply at the level of molecules and
chromosomes, and ignoring it is an immoral behavior,
and should not occur in the claimed era of human
rights and in the current advanced health and
war technology. We believe until proven otherwise,
that semi-nuclear is nuclear as well, and nucleotides
and genes do not read well these accumulative
quantitative gradients of radiology, but we do.
Scientific silence is a hypocritical act, and
it is the other face of the coin of death.
Table 1: The half-lives* and specific activity
of the 3 isotopes of Uranium
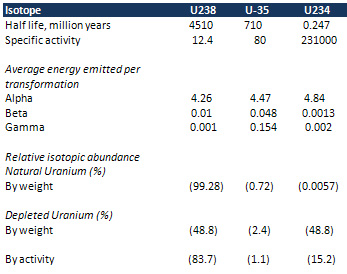
*The half life of a radioactive isotope is the
time needed to decay to half
of its original radioactivity
Hamdi H.
Shelleh. Depleted Uranium. Saudi Med J 2012; Vol.
33 (5):483-488.
|
