|
Diagnosis of Porphyria
after sternotomy for severe calcific coronary
artery disease, a Case Report
......................................................................................................................................................................
Fuad Alazzam (1)
Salah Altarabsheh (1)
Mohammad Khasawneh (2)
(1) MD, Division of Cardiovascular Surgery, Queen
Alia Heart Institute, Amman, Jordan
(2) MD, Division of Cardiac Anesthesia, Queen
Alia Heart Institute, Amman, Jordan
Correspondence:
Mohammad Khasawneh, MD
Queen Alia Heart Institute
Jordanian Royal Medical Services
Email: khasawneh03@yahoo.com
|
ABSTRACT
Acute intermittent porphyria (AIP) is an
autosomal disorder marked by a deficiency
of the enzyme, the hydroxymethylbilane synthase
which is part of the heme biosynthesis.
It is manifested clinically by multi-system
involvement. Our patient does have chronic
ischemic heart disease needed surgical revascularization;
his sternotomy incision revealed the classical
blackish discoloration of the bone marrow,
which guided us for his work up and diagnosis.
Key words: acute
intermittent porphyria (AIP), coronary artery
bypass grafting (CABG), left internal mammary
artery (LIMA).
|
Porphyria, a hematological disease,
which involves the heme metabolism, can present
with multiple features. It has many clinical presentations
which can mimic multiple diseases.
Here we present this case which was diagnosed
with acute intermittent porphyria (AIP) during
sternotomy for CABG.
We report a 40-year-old gentleman
who, apart from smoking history, had no other
risk factors for coronary artery disease. One
more pertinent issue is that he had a chronic
history of vague left loin pain which is intermittent
and was treated as urinary gravels. This gentleman
had recurrent attacks of angina chest pain, for
which he was studied in the cardiology clinic
and his work up included coronary angiogram which
revealed three vessel coronary artery disease
not amenable for percutaneous coronary intervention.
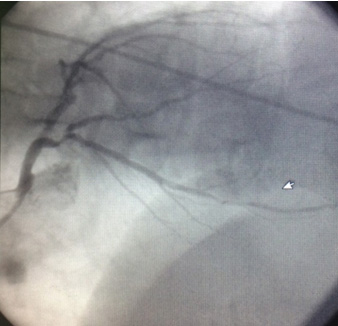
After reviewing his coronary angiogram, there
were multiple calcific lesions with variable distribution
along his coronary territories (Figure 1). Decision
was taken to operate on
him and perform coronary artery bypass grafting.
He was brought to the operating room for elective
triple coronary bypasses for his diseased coronaries.
Given his very young age, this raised the suspicion
of a systemic disease.
Figure 1: Coronary Angiogram revealing multiple
diffusely distributed calcific spots along the
coronary territories.
After being prepped and draped
in the usual sterile fashion, full primary median
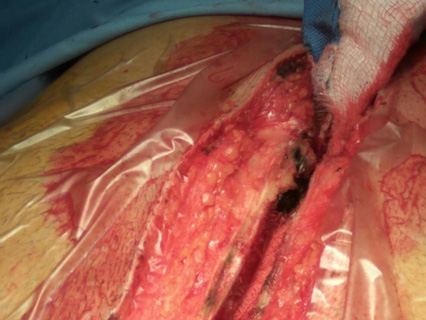
sternotomy was performed. Interestingly there
was a dark black colored bone marrow spot at the
distal lower part of the sternum (Figure 2), for
which, an incisional biopsy was sent to the histopathology
laboratory. During LIMA harvesting, multiple dark
black spots covering multiple ribs were also noted.
Figure 2: Intra-operative view, demonstrating
a blackish discolored spot in the lower aspect
of the sternotomy incision
When pericardium was opened and heart suspended
in pericardial cradle, cardiopulmonary bypass
was commenced at 2.4 L/M/M2 and patient temperature
drifted to 34 c. and cardioplegic arrest done
with ante grade and retrograde fashion. Coronary
arteries were examined and showed diffuse calcification
with multiple dark spots.
Surgery was uneventful and patient recovered fully
and was discharged 10 days after multiple diagnostic
tests were sent and confirmed his disease.
Many groups of disorders that
are due to accumulation of Porphyrins can produce
the disease of porphyria (1 ,2). It is inherited
as autosomal pattern - which is most common -
as well as autosomal recessive - rarely occurring
Porphyria's affect many organs including CNS,
skin, kidneys, liver and bone as well.
Vague presentations and lots of nonspecific signs
and symptoms make the diagnosis difficult in solitary
cases which have no family history of such a disease,
as in this case.
Triggering factors that might precipitate the
acute attacks of porphyria include alcohol, smoking,
medications, fasting, stressful events, infections
and others.
Other forms of porphyria can produce cutaneous
manifestations which is not in the scope of this
case.
Subtle changes of organ tissues
can be the stepping stone for the workup of rare
diseases. High index of suspicion and systemic
examinations of all tissues apart from the planned
interventions may make outcomes better. Our case
can serve as a reminder to keep these rare diagnoses
in mind when such a scenario may be faced.
1. Elena Pischik, Raili Kauppinen.
An update of clinical management of acute intermittent
porphyria. The Application of Clinical Genetics
2015, 8:201-214
2. Benassi F1, Righi E,
Cimato P, Parravicini R. Cardiac surgery in patients
with acute intermittent porphyria. J Card Surg.
2012 May;27(3):331-4
|
