|
Carpal tunnel
syndrome during pregnancy
......................................................................................................................................................................
Kholoud Abdelnabi
Correspondence:
Dr. Kholoud Abdelnabi
Specialist, Department of Obstetrics and Gynecology.
Royal Medical Services
Jordan
Mobile: 00962776134468
Email: mkateeb@lycos.com
|
ABSTRACT
Objectives: To assess the current
frequency of carpal tunnel syndrome during
pregnancy in our area and to assess the
course of carpal tunnel syndrome during
pregnancy in those patients.
Material and Methods: This is a prospective
study of 400 women attending antenatal outpatients'
clinic. This study was conducted between
the 1st of July 2009 and the end of August
2010 at King Hussein Medical Center, Jordan.
At each demographic details and issues related
to their problems were obtained.
Results: During the study period,
400 pregnant women attending antenatal outpatients'
clinic in our hospital, 74 (18.5%) women
were found to have carpel tunnel symptoms.
Most of them were in third trimester of
pregnancy 81.1% (no=60) followed by the
second trimester 16.2% (no=12) and the least
were in the first trimester 2.7% (no=2).
The most common complaint was numbness,
particularly during the daytime (78.4%),
while the least frequent symptom reported
was pain. However, about half of women with
CTS during pregnancy still complained of
CTS symptoms one year after delivery.
Conclusion: A large number of pregnant
women suffer from the frequent occurrence
of CTS in pregnancy and are first noted
during the third trimester, but only in
half of women CTS symptoms disappeared one
year after delivery.
Key words: Carpal tunnel syndrome,
pregnancy, prevalence.
|
Carpal tunnel syndrome (CTS)
is an entrapment median neuropathy, causing paresthesia,
pain, numbness, and other symptoms in the distribution
of the median nerve due to its compression at
the wrist in the carpal tunnel(1). Most cases
of CTS are of unknown causes, or idiopathic(2),
but CTS may be associated with trauma, and with
any condition that causes pressure on the median
nerve at the wrist. Some common conditions that
can lead to CTS include obesity, oral contraceptives,
pregnancy, hypothyroidism, arthritis and diabetes.
Up to one third of cases of carpal tunnel syndrome
occur in association with such medical conditions
(3). So Carpal tunnel syndrome is one of the most
common peripheral neuropathies, and is one of
the commonest elective clinical conditions presenting
to hand surgery departments(4).
Carpal tunnel syndrome is common during pregnancy
and is considered to have a short and benign course.
It occurs most frequently in the third trimester
but can develop at any time. Conservative therapies
for the patient with mild symptoms of CTS are
appropriate and common initial measures with very
few cases require surgery. The symptoms resolve
after delivery in most women with pregnancy-related
carpal tunnel syndrome(5). However, in moderate
to severe cases, surgery is the only treatment
that provides cure. The basic principle of surgery
is to increase the volume of the carpal tunnel
by dividing transverse carpal ligament to release
the pressure on the median nerve(6).
In the general population, the prevalence of CTS
is approximately 9.6%, approximately 2.3% to 4.6%
of patients with CTS are pregnant, and up to 50%
of all pregnant women have nocturnal hand symptoms,
mostly in the third trimester. Swelling in the
hand and wrist caused by fluid retention compresses
the median nerve. Also hormonal changes in pregnancy
may explain this increase because a similar predisposition
has been reported with menopause(7).
In spite of the public health importance of CTS,
there are no universally accepted diagnostic clinical
and laboratory criteria. However, it is agreed
that certain electrophysiological abnormalities
support the diagnosis. The most frequently used
parameters are distal motor and sensory latencies
as well as the sensory conduction velocity across
the carpal tunnel(8). The diagnosis of CTS is
traditionally based on clinical history, physical
examination results, and electrophysiologic study
results. More recently, ultrasonography (US) has
been shown to be an accurate and useful diagnostic
tool in patients with CTS(9).
The present study was undertaken with the aim
of assessing the current frequency of carpal tunnel
syndrome during pregnancy in our area in patients
attending this hospital in Jordan and to assess
the course of carpal tunnel syndrome during pregnancy.
This is a prospective study of
400 women attending antenatal outpatients' clinic.
This study was conducted between the 1st of July
2009 and the end of August 2010 at King Hussein
Medical Center, Jordan. The study was approved
by the ethics committee and informed written consent
from all participants was obtained.
History and clinical examination of the patients
was performed for all women. Maternal demographics,
obstetrical events, delivery outcome, previous
medical and surgical history were evaluated. All
the data were compiled and continuous variables
were analyzed using Student t-test. CTS were diagnosed
clinically based on patient history, physical
examination and electrophysiological findings.
The exclusion criteria include patients with diabetes
mellitus, gestational diabetes mellitus, eclampsia,
preeclampsia, thyroid disorders, trauma to the
hand or wrist, and prior history of CTS.
All the women who were found to have carpel tunnel
symptoms with electrophysiological proven CTS
were followed in the neurosurgical clinic throughout
their pregnancy and one year after delivery. Those
patients were treated in different modalities.
Symptoms follow up was done.
During the study period (2009-2010),
400 pregnant women attending antenatal outpatients'
clinic in our hospital, and 74 (18.5%) women were
found to have carpel tunnel symptoms and were
sent to the neurosurgical clinic. All of them
were subjected to nerve conduction study for objective
assessment of CTS, and electrophysiological test
proven CTS. So the current incidence of carpel
tunnel syndrome amongst women attending our hospital
was 18.5%. Most of them were in the third trimester
of pregnancy 81.1% (no=60) followed by the second
trimester 16.2% (no=12) and the least were in
the first trimester 2.7% (no=2).
The most common complaint was numbness, particularly
during the daytime (78.4%), while the least frequent
symptom reported was pain, especially pain that
awakened patients at night (16.2%) as seen in
Table 1.
In addition, the study revealed that neurophysiological
evaluation provided diagnosis of CTS in around
half of women (45% were positive in one hand at
least). Comparison of baseline and follow-up data
showed a significant spontaneous improvement of
patient-oriented and neurophysiologic measurements.
However, about half of women with CTS during pregnancy
still complained of CTS symptoms one year after
delivery, despite symptomatic and electrodiagnostic
improvement, 42% of patients still had diminished
median distal sensory conduction velocities.
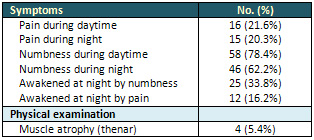
Table 1: Clinical findings among patients with
carpal tunnel syndrome (n = 74).
Carpal tunnel syndrome is a
disorder of the hand caused by pressure on the
median nerve as it runs through the wrist. During
pregnancy, hormonal fluctuations, fluid shifts,
and musculoskeletal changes predispose women to
carpal tunnel syndrome. In pregnancy hormonal
changes may result in fluid retention, which can
compress the median nerve. CTS triggered during
pregnancy usually resolves soon after birth. Symptoms
may be exacerbated by repetitive hand movements,
holding hands in sustained positions or by putting
weight through outstretched hands(10).
Existing data reports a prevalence of CTS in pregnancy
to be as high as 62%(11) and as low as 0.23%(12).
Most of these data are based on clinical symptoms.
Our findings were in agreement with those of a
study by Bahrami et al that showed that 17% of
pregnant women had CTS during pregnancy(13). Also
our findings were in agreement with those of a
study by Khosrawi et al(14) that showed that 63%
had CTS hand symptoms during their third trimester
of pregnancy, while in two other studies in the
third trimester; the prevalence was 28% and 43%(15,16).
However, unlike many studies, numbness and tingling
sensation were prominent symptoms in our study
of pregnant women with CTS(78.4%). Pain was reported
to be quite common among patients by other authors(17,18).
We found that the incidence of numbness/tingling
during daytime was slightly higher than at night
among the women, which is at odds with the classical
description of nocturnal paraesthesia in such
patients in many orthopaedic textbooks.
In our study, neurophysiological evaluation provided
diagnosis of CTS in around half of women (45%
were positive in one hand at least) as seen by
Padua et al study(19).
Almost all reported a short follow-up with disappearance
of symptoms. Our study confirms that pregnancy-related
CTS has a benign course: improvement of symptoms
was evident at one year follow-up, but about half
the women still complained of symptoms one year
after delivery as Mondelli et al(20) reported
that at one-year follow-up improved in 40% of
women, did not change in 46.7% and 55.6% and worsened
in 13.3% and 4.4%, respectively.
1. Andreisek G, Crook DW,
Burg D, Marincek B, et al. Peripheral Neuropathies
of the Median, Radial, and Ulnar Nerves: MR Imaging
Features. September 2006 RadioGraphics: 26, 1267-1287.
2. Sternbach G. "The carpal tunnel syndrome".
J Emerg Med. 1999 May-Jun; 17(3):519-23.
3. Katz JN, Simmons BP. Clinical practice. Carpal
tunnel syndrome. N Engl J Med. 2002 Jun 6; 346(23):1807-12.
4. Burke FD, Ellis J, McKenna H, Bradley MJ. Primary
care management of carpal tunnel syndrome. Postgrad
Med J. 2003 Aug; 79(934):433-7.
5. Jurjevic A, Bralic M, Antoncic I, Dunatov S,
et al. Early onset of carpal tunnel syndrome during
pregnancy: case report. Acta Clin Croat. 2010 Mar;
49(1):77-80.
6. Aroori S, Spence RA. Carpal tunnel syndrome.
Ulster Med J. 2008. Jan; 77(1):6-17.
7. Stolp-Smith KA, Pascoe MK, Ogburn PL Jr. Carpal
tunnel syndrome in pregnancy: frequency, severity,
and prognosis. Arch Phys Med Rehabil. 1998 Oct;
79(10):1285-7.
8. Verdugo RJ, Salinas RS, Castillo J, Cea JG. Surgical
versus non-surgical treatment for carpal tunnel
syndrome. Cochrane Database Syst Rev. 2008 Oct 8;
(4):CD001552.
9. Klauser AS, Halpern EJ, Faschingbauer R, Guerra
F, et al. Bifid median nerve in carpal tunnel syndrome:
assessment with US cross-sectional area measurement.
Radiology. 2011 Jun; 259(3):808-15.
10. Werner RA, Andary M. Carpal tunnel syndrome:
pathophysiology and clinical neurophysiology. Clin
Neurophysiol. 2002 Sep;113(9):1373-81.
11. Ablove RH, Ablove TS. Prevalence of carpal tunnel
syndrome in pregnant women. WMJ. 2009 Jul; 108(4):194-6.
12. Stolp-Smith KA, Pascoe MK, Ogburn PL Jr. Carpal
tunnel syndrome in pregnancy: frequency, severity,
and prognosis. Arch Phys Med Rehabil. 1998 Oct;
79(10):1285-7.
13. Bahrami MH, Rayegani SM, Fereidouni M, Baghbani
M. Prevalence and severity of carpal tunnel syndrome
(CTS) during pregnancy. Electromyogr Clin Neurophysiol.
2005; 45(2):123-5.
14. Khosrawi S, Maghrouri R. The prevalence and
severity of carpal tunnel syndrome during pregnancy.
Adv Biomed Res. 2012;1:43.
15. Ordbieg G. Carpal tunnel syndrome in pregnancy.
Acta Obstet Gynecol Scand 1987;66:235-7.
16. Pazzaglia CC. Multicenter study on carpal tunnel
syndrome and pregnancy incidence and natural course.
Asta Neuro Chir Suppl 2005;92:35-9.
17. Baumann F, Kar I ikaya, Yuksel G, et al. The
subclinical incidence of CTS in pregnancy: assessment
of median nerve impairment in asymptomatic pregnant
women. Neurol Neurophysiol Neurosci 2007:3.
18. Stolp-Smith KA, Pascoe MK, Ogburn PL Jr. Carpal
tunnel syndrome in pregnancy: frequency, severity,
and prognosis. Arch Phys Med Rehabil. 1998; 79:1285-7.
19. Padua L, Aprile I, Caliandro P, et al. Symptoms
and neurophysiological picture of carpal tunnel
syndrome in pregnancy. Clinical neurophysiology
112 (2001):1946-1951.
20. Mondelli M, Rossi S, Monti E, Aprile I, et al.
Long term follow-up of carpal tunnel syndrome during
pregnancy: a cohort study and review of the literature.
Electromyogr Clin Neurophysiol. 2007 Sep;47(6):259-71.
|
