|
The Importance
of Daily Routine Chest Radiography in Mechanically
Ventilated Children
......................................................................................................................................................................
Ahmed Alissa
Correspondence:
Ahmed Alissa, MD
Department of pediatrics
Queen Rania AL-Abdullah Hospital for Children
Royal Medical Services
P O BOX 855100
Postal code 11855
Amman, Jordan
Email: aalissa68@yahoo.com
|
ABSTRACT
Objective: To asses the usefulness
of daily routine chest radiography in mechanically
ventilated children.
Methods: This retrospective
study was conducted in a pediatric intensive
care unit at Queen Rania Al-Abdullah Hospital
for children during the period between February
1 and April 30, 2010. The chest radiographs
of 25 patients who had been mechanically
ventilated during the study period were
reviewed using the picture archiving and
communication system.
Results: Of the
25 patients, 13 (52 %) were males and 12
(48 %) were females. The age ranged between
1 day and 14 years of life. 245 chest radiographs
were evaluated by a pediatric intensivist.
23 % of all radiographs showed cardiopulmonary
abnormalities, 12 % showed malpositioned
endotracheal tubes and 9 % malpositioned
central venous catheter. 14% of chest radiographs
had findings that altered management. The
most frequent management changes done were
repositioning of central venous catheters,
and changes in drug therapy.
Conclusion: We conclude
that the daily routine chest radiography
in mechanically ventilated children had
diagnostic and clinical usefulness.
Key words:
pediatric, Intensive care, chest radiography,
Intubation.
|
The portable chest roentgenogram
is one of the most frequent and effective diagnostic
examinations used in the intensive care unit (1).
Obtaining daily routine chest-X Ray is a labor-intensive
strategy, while diagnostic and therapeutic yields
of daily routine chest-X Rays are low (2). Chest
radiographs are routinely obtained in critically
ill patients to monitor both clinical condition
and to evaluate placement of invasive instruments
such as central venous catheters and endotracheal
tubes (3).
The consensus opinion of the American College
of Radiology Expert Panel is that daily routine
chest radiographs are indicated in patients with
acute cardiopulmonary problems and in patients
receiving mechanical ventilation (4).
This retrospective study was
conducted in a pediatric intensive care unit at
Queen Rania Al-Abdullah Hospital for children
during the period between February 1 and April
30, 2010. The Queen Rania AL-Abdullah Hospital
for Children is one of the affiliated hospitals
of King-Hussein Medical Center in Amman, Jordan.
The pediatric intensive care unit is an 18 bed
mixed medical-surgical unit admitting children
from birth to 14 years of age. Portable chest
radiographs are routinely done every morning at
8 AM for mechanically ventilated children. Chest
radiographs which are done when clinically indicated
are called on demand chest X-Rays. The indication
for on demand chest X-Rays includes placement
of central venous catheters, endotracheal intubation
and chest tube drain insertion. The chest radiographs
are reviewed on daily morning rounds by pediatric
intensive care consultant and fellows. These chest
radiographs are accessible in the picture archiving
and communication system (PACS) to the attending
physicians.
Of the 25 patients, 13 (52 %)
were males and 12 (48 %) were females. Age ranged
between 1 day and 14 years of life. Over a three
month period 245 chest radiographs were done for
25 mechanically ventilated children. The main
causes of admissions are shown in Table 1. 23
% of all radiographs showed cardiopulmonary abnormalities,
12 % showed malpositioned ET tubes and 9 % malpositioned
CVC. 14% of chest radiographs had findings that
altered management. The most common management
changes were repositioning of CVC and changes
of drug treatment.
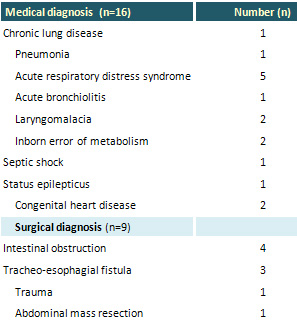
Table 1: The Main diagnoses of the study group
(n =25)
Whether chest radiographs in
mechanically ventilated patients should be routinely
obtained or only when an abnormality is anticipated
remains debated (5).
While most medical studies evaluating daily chest
X-Rays in patients in the ICU have been in adult
populations, a few on children are available (3).
Our study showed that 14% of chest X-Rays had
findings that changed management in the form of
antibiotic coverage and repositioning of CVC.
These results indicate clinical and diagnostic
usefulness of daily routine chest X-Rays in mechanically
ventilated pediatric patients.
Previous studies have evaluated the efficacy of
daily routine chest X-Rays in mechanically ventilated
children.
Sivit CJ et al prospectively evaluated the efficacy
and clinical usefulness of bedside chest radiography
in a pediatric intensive-care unit, where seven
hundred and ninety-five radiographs were evaluated
in 126 patients over a 10-week period in Children's
Hospital National Medical Center, Washington,
D.C and their data indicated that bedside radiography
in the pediatric intensive-care setting has a
high efficacy and clinical utility (6).
Brainsky et al observed that 20% of routine chest
X-Rays performed in a medical ICU had major important
findings, and 8% prompted a change in management.
The majority of changes related to diuretic use,
antibiotic coverage, initiation of a diagnostic
test, or decisions regarding ventilator weaning
(7).
In a prospective study, Hall et al compared bedside
clinical diagnosis with the diagnosis made from
the routine chest X-Ray. A total of 538 chest
radiographs were examined; of these, 354 (65.8%)
did not disclose either new major or new minor
findings but one hundred and sixty-three radiographs
disclosed only new minor findings, 40.5% of which
were anticipated by bedside assessment (8). However,
in 13 (17.6%) of the 74 patients, new major findings
were discovered only by chest radiography. These
data demonstrate that, while a large percentage
of radiographs will not disclose new findings,
routine daily studies have a substantial impact
on the management of intubated, mechanically ventilated
patients in the ICU which support the use of daily
chest radiographs in critically ill patients (8).
On the contrary to the findings of our study,
many studies have questioned the usefulness of
daily routine chest X-Rays on diagnostic and therapeutic
level and its association with economic cost.
A study conducted by Karine A et al in Amsterdam-Netherland
on 1780 daily routine chest-X-Rays in 559 hospital
admissions, reported low value of daily routine
chest-X-Rays (2).
Hejblume G et al compared
routine and on-demand chest radiography in 21
intensive care units at 18 hospitals, in France.
They strongly support adoption of an on-demand
strategy in preference to a routine strategy to
decrease use of chest radiographs in mechanically
ventilated patients without a reduction in patients'
quality of care or safety(9).
Bekemeyer et al found that 27% of both routine
and non-routine chest-X-Rays revealed clinically
unsuspected abnormalities, but that non-routine
films were more likely to change investigative
or therapeutic management (10).
Price et al found that 37% of chest-X-Rays could
be avoided by establishing specific indications,
thereby resulting in significant cost savings
(11).
Chahine-Malus N et al evaluated the diagnostic
and therapeutic efficacy of daily routine and
clinically indicated chest-X-Rays in a prospective
controlled blinded study in a nonacademic, mixed
medical-surgical ICU., In addition, the effects
of abandoning the daily routine chest X-Rays strategy
on chest Ray volume, ICU length of stay, readmission
rate, and mortality were evaluated during a 6-month
period. The results confirm and corroborate previous
data indicating that the diagnostic yield and
therapeutic consequences of daily routine chest-
X-Rays are very low (12).
In summary we conclude that daily routine chest
radiographs in mechanically ventilated children
had diagnostic and therapeutic usefulness but
we need a study to compare between daily chest
X-Rays and on demand chest X-Rays with more patients
to be included and figures to be statistically
analyzed to support our opinion.
1- Ganapathy A , Adhikari
N , Spiegelmon J et al. Routine chest x-rays in
ICU : a systematic review and meta-analysis. Critical
Care 2012, 16 : R68 .
2- Hendriske K, Gratama J, Hove W et al. Low value
of routine chest radiographs in a mixed medical-surgical
ICU. Chest 2007; 132: 823-828.
3- Levy F, Bratton S, Jardine D. Routine chest radiography
following repositioning of endotracheal tubes are
necessary to assess correct position in pediatric
patients. Chest 1994; 106: 1508-1510.
4- Gratt M, Choi G, Wolthuis E et al. The clinical
value of daily routine chest radiographs in a mixed
medical-surgical intensive care unit is low. Critical
care 2006; LO (1): R 11.
5- Clech C, Simon P, Hamdi A et al. Are daily routine
chest radiographs useful in critically ill, mechanically
ventilated patients? A randomized study. Intensive
care med 2008; 34(2): 264-270.
6- Sivit C, Taylor G, Hauser G et al. Efficacy of
chest radiography in pediatric intensive care. Am
J Roentgenol 1989; 152: 575-577.
7- Brainsky A, Fletcher RH, Glick HA et al. Routine
portable chest radiographs in the medical intensive
care unit: effects and cost. Crit care med 1997;
25: 801-805.
8- Hall B, White SR, Karrison T. Efficacy of daily
routine chest radiographs in intubated mechanically
ventilated patients. Crit care med 1991; 19: 689-693.
9- Hejblum G, Chalumear-Lomoine L, Loose V et al.
Comparison of routine and on-demand prescription
of chest radiographs in mechanically ventilated
adults: a multicenter, cluster-randomized, tow-period
crossover study. Lancet 2009; 374 (9702): 1687-1693.
10-Bekemeyer WB, Crapo RO, Calhoens et al. Efficacy
of chest radiography in a respiratory intensive
care unit. Chest 1985 ; 88: 691-696.
11-Price MB, Chellis MJ, Welkie K. Financial impact
of elimination of routine chest radiographs in a
pediatric intensive care unit. Crit care med 1999;
27: 1588-1593.
12-Chahine N, Stewart T, Lapinsky et al. Utility
of routine chest radiographs in a medical-surgical
intensive care unit: a quality assurance survey.
Critical care 2001; 5: 271- 275.
|
